Medication Management: IV Ketamine when taking other medications

Schedule Your Ketamine Therapy Consultation Today
People considering ketamine for their mental health often ask:
“Is it safe to take my current medications with IV ketamine, and will they interfere with ketamine’s antidepressant effects?”
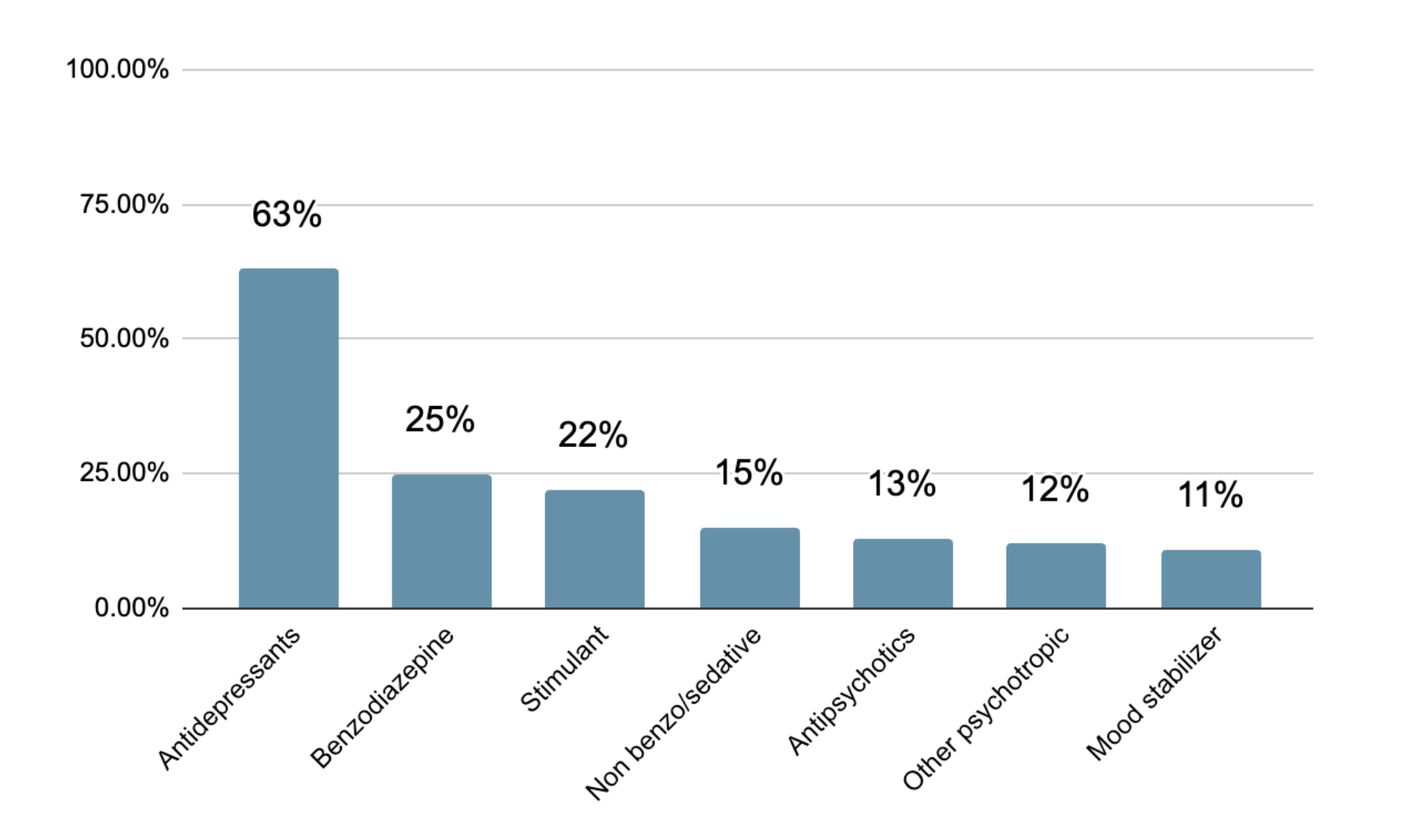
At Ember Health, medication management is central to how we deliver safe, effective care. Most individuals who pursue IV ketamine are already taking other medications for their mental health. Many have been in treatment for years, where antidepressants, benzodiazepines, mood stabilizers, stimulants, or antipsychotics are often part of a carefully constructed treatment plan.
The highest level take-away is that ketamine is safe to take with other medications. There are no medication combinations that present dangerous or life-threatening interactions with ketamine. There is some evidence, however, that suggests that some types of medications may inhibit the antidepressant effect of IV ketamine. Understanding how these medications interact with ketamine allows us to optimize outcomes while preserving safety and continuity of care.
This article explains how Ember approaches medication management, what the scientific literature tells us about potential interactions, what guidance we provide in practice, and what we’ve learned from our own large-scale research collaboration with Harvard Medical School and Mass General Brigham.
This article is intended for informational and educational purposes only, and does not constitute medical advice, diagnosis, or treatment; medication decisions should be made in consultation with a qualified healthcare professional who can evaluate your individual medical history and clinical circumstances.
A Partnership-Based Model of Care
Ember operates under a collaborative, partnership-based treatment model. We are not a patient’s primary mental health provider, and we do not independently diagnose depression nor do we assume prescription medication management. Instead, every patient in our care must have an outside licensed mental health clinician who:
- Establishes and maintains formal psychiatric diagnoses
- Prescribes and manages any non-ketamine ongoing medications
- Collaborates with us for care
We only start care once this framework is in place. That structure allows us to focus specifically on IV ketamine while ensuring that broader medication management remains consistent and medically supervised.
Many patients hope that successful ketamine treatment may eventually allow them to reduce certain medications, particularly antidepressants. When that goal is clinically appropriate, we work closely with the prescribing clinician to ensure any taper is gradual, thoughtful, and safe. Medication changes are never abrupt, and they are never made independently by Ember without coordination.
This model empowers ketamine to function as an integrated component of care.
What the Scientific Literature Shows
The broader research landscape is reassuring. A comprehensive review published in Frontiers in Psychiatry (Zarate et al., 2021) examined pharmacological interactions between ketamine and commonly prescribed psychiatric medications. The overall conclusion was clear: ketamine is generally safe when used in conjunction with most psychotropic medications.
This is a meaningful distinction from certain serotonergic psychedelic compounds currently in research trials, such as psilocybin and other classic psychedelics, which primarily act as serotonin receptor agonists. These treatments have previously required medication washouts due to the concerns around serotonin syndrome, as well as concerns that SSRIs/SNRIs may attenuate their therapeutic effects. This has means that meaning it is potentially not safe, or effective, to engage in such psychedelic treatments while actively using most antidepressant medications. Ketamine on the other hand, does not meaningfully elevate serotonin levels, has not been associated with dangerous serotonergic toxicity when combined with SSRIs or SNRIs, and doesn't appear to be blunted by standard antidepressants.
Researchers have examined ketamine alongside multiple medication classes, including:
- SSRIs and SNRIs
- Tricyclic antidepressants and MAO inhibitors
- Antipsychotics
- Mood stabilizers such as lamotrigine
- Benzodiazepines
- Other GABAergic agents
- Naltrexone
- Stimulants
Across decades of clinical practice, ketamine has demonstrated broad safety and compatibility. With that being said, a few medication categories have generated more nuanced discussion.
Benzodiazepines — such as lorazepam, clonazepam, or alprazolam — are the most frequently debated medications in the ketamine literature. Some observational studies suggest benzodiazepines may blunt the antidepressant effects of ketamine, particularly at higher doses. A few dose-response analyses indicate that individuals taking larger benzodiazepine doses may experience somewhat smaller improvements. However, these findings are mixed and largely derived from non-randomized data.
Importantly, even in studies suggesting attenuation, ketamine still demonstrated meaningful antidepressant benefit. The concern is not that benzodiazepines negate ketamine’s effects, but that high doses might reduce the magnitude of effect in certain individuals.
Other medications have been carefully considered for their potential interaction with IV ketamine:
- GABA-related agents (non-benzodiazepines, like Gabapentin): Limited data, but theoretical potential to dampen the antidepressant effect.
- Lamotrigine (Lamictal): Some reports suggest it may blunt the subjective altered-state experience; evidence for reduced antidepressant efficacy is mixed.
- Naltrexone: Data are inconsistent regarding its impact on ketamine’s mechanism.
- Antidepressants: SSRIs and SNRIs do not appear to diminish ketamine’s effectiveness.
- Mood stabilizers: Do not appear to diminish ketamine’s effectiveness.
Overall, the scientific literature supports ketamine’s safety and compatibility across these psychiatric medication classes.
The Practical Guidelines We Provide at Ember
While ketamine is broadly compatible with psychiatric medications, we provide structured, conservative guidance designed to optimize therapeutic outcomes in coordination with each patient’s prescribing clinician. The general statements in this article do not replace the careful conversations with your prescribing provider.
Ketamine therapy offers evidence-based treatment for depression, anxiety, and other mental health conditions. Schedule a consultation call to learn more.
- Brooklyn Heights
- Chelsea
- Tribeca
- Upper East Side
- Williamsburg
For benzodiazepines, our general approach emphasizes dose optimization rather than abrupt discontinuation. We typically recommend:
- Using the lowest tolerable dose
- Avoiding sudden discontinuation to prevent withdrawal
- When possible, avoiding use within 24 hours before and after an infusion
- Exceptions exist for longer half-lives in medications like clonazepam, which ideally are avoided for 36 hours before and after an infusion
The rationale is partly neurobiological and partly experiential. Benzodiazepines impair memory consolidation, and some of ketamine’s therapeutic benefits may relate to psychological processing and integration.
For other medications:
- GABAergic sedatives are ideally avoided within 24 hours of infusion when feasible
- Lamotrigine is typically held within six hours prior to an infusion to preserve experiential immersion, then resumed as scheduled
- Naltrexone management is individualized based on the reason it is prescribed
These recommendations are conservative, and aim to preserve ketamine’s therapeutic window without destabilizing the broader treatment plan.
What We've Learned from Our Own Research
While existing literature is helpful, we wanted to understand how medication interactions function in real-world practice within a structured care model.
In collaboration with Harvard Medical School and Mass General Brigham, Ember conducted a large retrospective study under IRB approval examining 2,097 adult patients treated with our structured four-infusion Foundation of Care protocol over 14 days.
Patients had significant baseline depression severity (average PHQ-9 of 16). The majority had comorbid Anxiety, PTSD, or other mental health issues
Across the cohort, patients demonstrated rapid and clinically meaningful reductions in depressive symptoms.
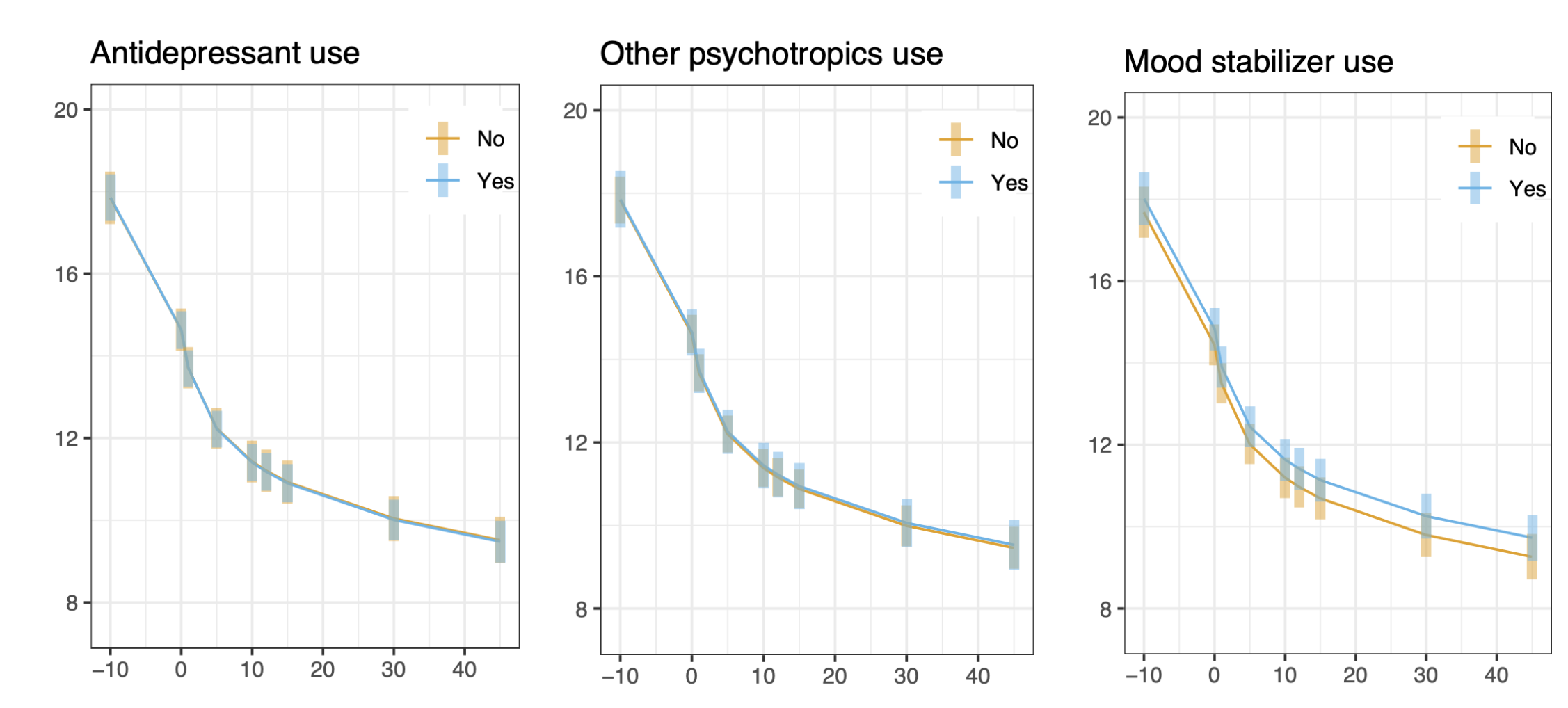
When examining medication categories more closely, several findings emerged.
- Antidepressants did not reduce ketamine’s effectiveness. Mood stabilizers similarly showed no meaningful reduction in Ketamine’s antidepressant benefits.
- Patients taking benzodiazepines began treatment with higher pre-treatment depression scores and ended treatment with higher scores as well. However, the rate of improvement over time — the slope of response — was not significantly different. In other words, within our structured medication-guidance model, benzodiazepines did not appear to blunt ketamine’s antidepressant effect.
- Antipsychotics and non-benzodiazepine sedatives showed a similar pattern: higher baseline severity before and after treatment, but meaningful improvements from treatment.
- Perhaps most intriguingly, use of stimulants showed a trend toward faster antidepressant response. While this finding requires prospective study, it raises interesting mechanistic questions worth further investigation about whether stimulants can improve ketamine antidepressant effects.

Implications for Patients
What does this mean for someone considering IV ketamine? Practically speaking:
- Patients do not need to discontinue antidepressants to receive ketamine.
- Taking benzodiazepines does not disqualify someone from care. Thoughtful dose optimization and prescription coordination appear to maintain ketamine’s benefits.
- Medication management should be collaborative, structured, and individualized to each person going through care.
Our data reinforce a reassuring conclusion: ketamine produces safe, clinically meaningful antidepressant effects across medication categories when delivered within a coordinated care model.
A Thoughtful Integration
Depression treatment rarely exists in isolation. Most patients arrive with years of treatment history and complex medication regimens. Effective ketamine care must account for that reality.
At Ember Health, medication management is woven into the foundation of our approach. Through collaborative partnerships, evidence-based guidance, and ongoing research, we aim to preserve both safety and efficacy.
Ketamine does not require abandoning prior treatment. In many cases, it works alongside other medications. Sometimes, over time, ketamine allows thoughtful simplification of other prescriptions.
If you are considering IV ketamine or are currently in care and have questions about your medications, our clinical team is available to review them in coordination with your prescribing provider.
Thoughtful medication management matters, and when approached carefully, it supports — rather than limits — the antidepressant potential of IV ketamine.
To view the full ASKP presentation where Dr. Nico Grundmann presented this data, see the video below.


